TPO: Triple Pelvic Osteotomy
- Triple pelvic osteotomy (PPT) is surgery to correct hip dysplasia in non-arthritic animals.
- It is practised in animals generally aged from 8 to 12 months.
- It allows a rapid disappearance of lameness and strongly limits the development of osteoarthritis.
- It is a relatively cumbersome procedure, but it gives excellent results in 90% of cases, provided the indication is correctly stated.
Introduction
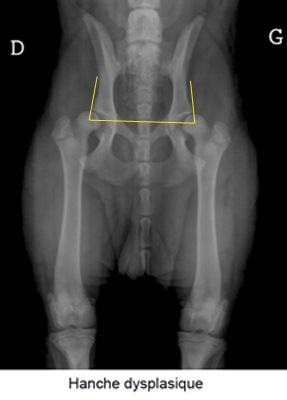
Coxofemoral dysplasia (hip dysplasia) is a common condition affecting mainly large breed dogs. This disease is due to abnormal development of the hip during the growth of the puppy. Heredity is a major factor in dysplasia. The parents may be nevertheless free from dysplasia, but they still have genes of the disease.
The first stage of hip dysplasia causes laxity of the hip joint. When the hip is supported, the hip becomes subluxated and as a result, the femoral head and the acetabulum (joint cavity) gradually deform as they flatten. Osteoarthritis appears on the joint and causes pain.
Sometimes the joint can be so altered that as a result of minor trauma it can dislocate. The animal then suddenly begins to limp. Most often, the condition is bilateral.
Generally, clinical signs of coxofemoral dysplasia can be detected around the age of 4 months, but diagnosis is more often made around 8 to 12 months. The main clinical signs are intolerance to exercise, gait, lameness, pain in hip extension, difficulty getting up after rest and atrophy of the muscles in the hindquarters. Some dogs do not show the first signs of dysplasia until around 2 years of age, or even when they are older after the onset of osteoarthritis.
The diagnosis of hip dysplasia is based on the combination of the animal's history, clinical signs present, orthopaedic and radiographic examinations. The operating decision is not made solely based on the radiographic examination, but takes into account the clinical context and the reality of the disability: "X-rays are not operated on".
The candidate for a triple osteotomy must have hip dysplasia, without osteoarthritis, a positive Ortalani sign (orthopaedic manoeuvre which makes it possible to highlight the laxity) with an angle of reduction lower than 40°, and especially the acetabulum must be retentive (the femoral head must enter the acetabulum in the radiographic position known as the frog). All candidates with a coxa-plana (flat cup), congenital hip dislocation or filled cup should be excluded from pat TPO therapy.
The procedure of the intervention
The principle of the operation is to make three cuts on the pelvic bone (triple osteotomy) to mobilise the acetabulum and tip it forward. This tilting effect increases the femoral head's dorsal overlap through the acetabulum and stabilizes the hip by neutralizing subluxation.
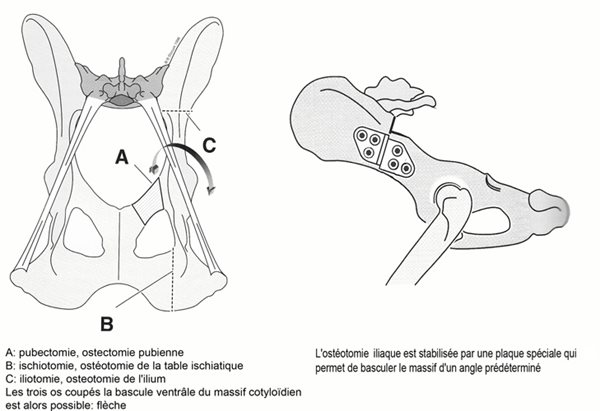
The intervention is carried out in three stages:
- Pubectomy: which consists of an inguinal approach to remove a small piece of the rising branch of the pubis
- The ischiotomy: consists of a caudal approach in cutting the ischiatic table in the sagittal plane.
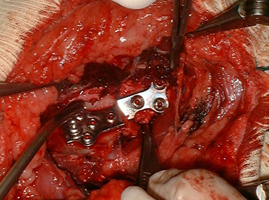
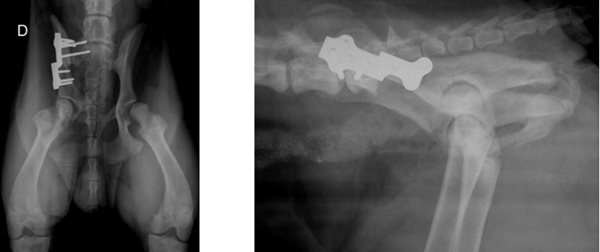
- The iliotomy: by the lateral approach of the ilium, a transversal section of the ilium is created which allows the acetabulum to be freed and tilted ventrally. This osteotomy is stabilized by a preformed osteosynthesis plate for triple pelvic osteotomy which allows giving exactly the desired angle of rotation.
1. 3.
3.
After the operation, the patient must be strictly confined for 45 days, the resumption of pressure on the operated limb normally occurs in the first post-operative week, and lameness normally disappears in less than three weeks. Radiological normalization with progressive hip stabilization is performed over approximately three months to obtain optimal coverage.
Treatment Effectiveness
Triple pelvic osteotomy when indicated gives excellent results with normalization of gait and suppression of lameness.
Arthritic development is slowed and will normally be negligible and without functional consequences.
Most operated animals have a normal life without deficit on the operated hips, the operation can be bilateral.
This is the hip dysplasia correction procedure that is the most performed and favoured by most surgeons. It is a regulated surgical procedure for which the recoil and evolution of the implants currently guarantee the patient the best chances of an optimal quality of life if the surgical indication is correctly placed.
TPO is a complex procedure that requires advanced practice and knowledge of orthopaedic surgery.
Possible complications
- Regardless of the technique, the risk of anaesthesia accident, however low, remains non-zero.
- Surgical site infections are rare, and strict adherence to aseptic rules in orthopaedic surgery can prevent them.
- Too much activity during the healing period may lead to loosening of the implants, surgical resurfacing may be necessary but most of the time the bone segments position correctly and the acetabular cover remains satisfactory. After 6 weeks the healing is normally advanced enough for the implants to move.
- Trauma to the sciatic nerve may occur during the procedure, the neurological deficit is usually transient and resolves in less than three weeks. Exceptionally an irreversible lesion can occur, its consequence is catastrophic with a permanent loss of use of the limb.
- Trauma to the pelvic urethra can also occur, resulting in transient hematuria.