Cauda Equina : Horsedick (Ponytail Syndrome)
- It is a pathology affecting the most caudal part of the lumbar spine and is comparable to the pathology of the sciatic nerve in men.
- It leads to a compression of the roots of the sciatic nerve which causes pain and locomotor disorders.
- The causes are varied: a herniated disc, narrow channel syndrome, vertebral instability, fracture, infection of the intervertebral disc, tumour...
- The evolution of ponytail syndrome (PTS) is normally chronic but acute forms may also exist.
- The SQC affects rather large breed dogs (German Shepherd, Labrador...) but toy dogs or cats can also be affected.
- Surgical treatment is effective if patients are operated on as early as possible before degenerative nerve damage occurs.
Introduction
Ponytail syndrome is a pathology of the lumbosacral junction and the caudal lumbar spine, it concerns regions of the spinal column after the end of the spinal cord for which only the nerve roots of the sciatic and sacral nerves exist, it is a pathology called the root stage.
It normally reaches animals of middle to advanced age and evolves in a chronic mode with a progressive degradation of motor skills and sensitivity in the territories of the sciatic nerve. However, early progression in the case of congenital malformations or acute presentations in the case of trauma or herniated discs is also possible. SQC is always accompanied by pain on the lumbosacral level, which is largely responsible for the animal's discomfort.
Anatomical elements and symptomatology
Compression concerns so-called root areas of the spine. Because of a growth differential during development, the spinal cord grows less than the spine, so there is a gap between the spinal and spinal segments. This shift is noticeable from the second lumbar vertebra (L2) and has as a consequence the end of the marrow (medullary cone) opposite the 5th lumbar vertebra. On the other hand, the spinal nerves continue to leave the vertebral canal through their respective foramens at the level of their corresponding vertebral segment. Thus, beyond L5-L6, only the nerves and the terminal part of the meninges (dural cone) remain, which by their filament aspect constitute the ponytail.
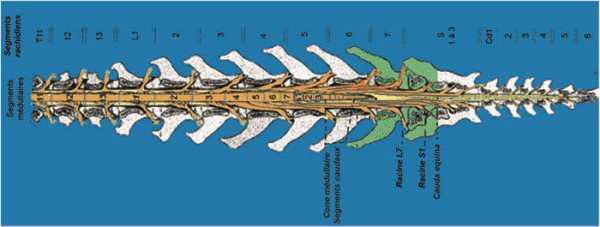
Cross-section view in the frontal plane of the terminal spine: notice the medullar cone facing L5 and L6 and beyond the medullar canal occupied only by nerves (oranges) stretched like the hairs of a ponytail.
Schematically, after leaving the spinal canal, the nerve bundles group together to form the sciatic nerve (roots L6 to S1) and the pelvic and shameful nerves (roots S1-S3). As a result, the intra-channel compressions after the sixth lumbar vertebra will result in nervous disorders on the sciatic nerves and pelvic nerves. Carnivore ponytail syndrome is equivalent in some ways to sciatica in humans.
The causes of compression of the ponytail are numerous, the lumbosacral junction (L7-S1) is a hinge zone of the spine with the connection of the spinal column to the pelvis via the sacrum. It is an area subject to significant mechanical stresses in bending and extension.
Congenital stenoses of the vertebral canal: the vertebral canal is too narrow and compresses the nervous tissue, these stenoses can be associated with malformations of the spine: the sacralization of the last lumbar vertebra, non-union of the sacral vertebrae... Congenital stenosis may have pathological consequences only late with the ageing of ligament structures and their thickening.
- Spinal instabilities: spondylolisthesis L7S1 for example.
- Herniated discs posterior to the end of the medullary cone.
- Intervertebral disc infection: spondylodiscitis, lumbosacral discospondylitis.
- Neoplasms of the spine or nerve tissue.
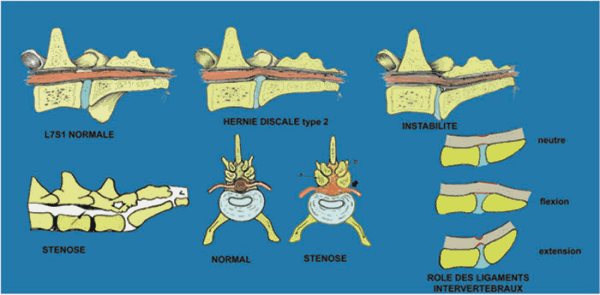
Major Non-Tumor Causes of Ponytail Syndrome
The symptoms are varied and their progressive appearance, most of the time the ponytail syndrome evolves on a chronic mode with a progressive degradation of the patient, exceptionally the evolution can be made on an acute mode in particular in case of an acute herniated disc or vertebral fracture/dislocation. The progression is often insidious.
- Pain at the lumbosacral junction is normally constant in ponytail syndrome and for a long time the only symptom present, this pain should not be confused with that which may be caused by coxofemoral dysplasia.
- A proprioceptive deficit on the hind legs results in excessive wear of the claws and scraping of the ground.
- Posterior ataxia.
- Muscular cast iron on the hind limbs.
- Decreased sciatic reflexes (withdrawal reflex and possibly patellar pseudo-hyperreflexia).
- Atony of the tail.
- Urinary and/or faecal incontinence in the most advanced cases.
The procedure of the intervention
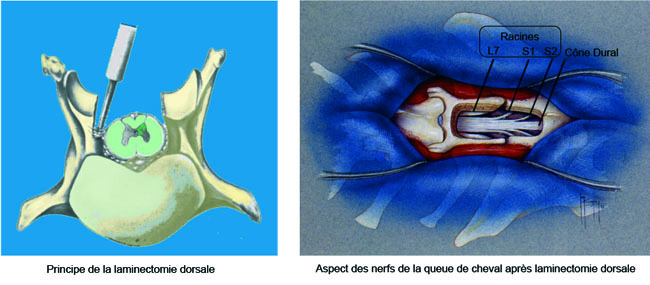
The operation is done under general anaesthesia, it consists in decompressing the nerve roots.
The most common procedure is a dorsal laminectomy of the L7 and S1 vertebrae (recalibration). This laminectomy can be extended to intervertebral foramens and joint apophyses to extend decompression to the roots in their foraminal path. Except in the case of a vertebral fracture, no additional stabilisation is generally performed in veterinary surgery. A discectomy (removal of the intervertebral disc) is also performed during the procedure in most cases.
In certain cases, notably when a very large laminectomy with extension to the intervertebral joints must be performed in order to treat intervertebral foramen stenosis or, in case of the existence of a very important spondylolisthesis, a complementary stabilisation of the spine must be performed. This is carried out by the installation of pedicle screw systems and union bars or locked titanium plates. These implants block the spinal movements and allow a faster recovery by facilitating the fusion of the vertebral bodies.
Lousewort screwing by Axon Synthes system after extended L7S1 laminectomy
for herniated disc with foraminal stenosis


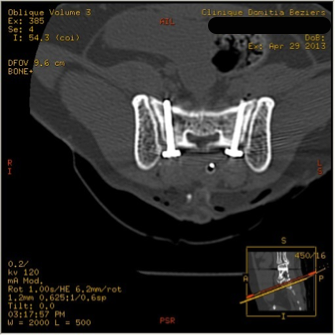
Lumbosacral stabilisation by pedicle screw and Unilock Synthès plates in a cat
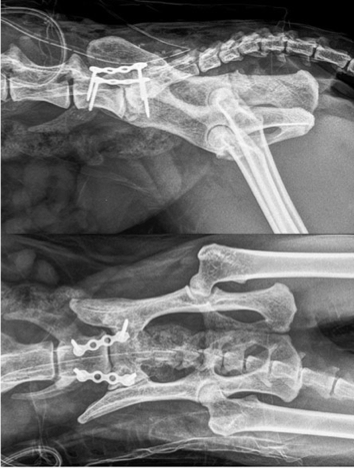
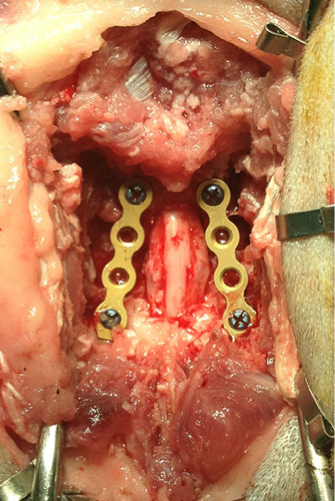
Stabilisation of lumbosacral junction after laminectomy and bilateral foraminectomy in a cat by pedicle screws and Unilock Synthès plates

Alternatively to dorsal laminectomy, an intervertebral arthrodesis in flexion can be performed, this technique is very rarely practised in France where the majority of surgeons prefer dorsal decompression.
Treatment Effectiveness
For animals operated early the effectiveness of the treatment is excellent with 90% good results. The pain is eliminated immediately and the locomotor disorders disappear within a few weeks. Patients regain the comfort of living and walking perimeter they had lost.
In advanced cases in which neurological degeneration is already present, the improvement is noticeable; however, some permanent nerve lesions cannot be recovered, but the evolution of the degenerative process is stopped.
From a postoperative point of view, at the root level, there is little or no motor impairment in the immediate postoperative period and patients are usually ambulatory the day after the operation.
Possible complications
- Regardless of the technique, the risk of accident to anaesthesia, however low, remains non-zero.
- Surgical site infections are rare and generally benign.
- A serous collection can be built up on the surgical site without functional consequences.
- Exceptionally a trauma of the nerve roots can intervene, this one can have catastrophic consequences.